Full HTML
Case Study of NMDA Encephalitis in an 18-Year-Old Female With No Underlying Etiolog. - Volume 1 Issue 2 (July-Dec), - (6 Months )
Pages: 4-10
Category: Short Report
Published Date: 21-11-2024
Sabina Nayab1, Qasim Bashir2, Adnan Aslam3, Amina Saeed khan4
Author Affiliation:
¹ Dr. Sabina Nayab, Postgraduate Resident, Department of Neurology, Services Hospital, Lahore, Pakistan.
² Prof. Dr. Qasim Bashir, Professor & Head, Department of Neurology, Services Hospital, Lahore, Pakistan
³ Dr. Adnan Aslam, Associate Professor, Department of Neurology, Services Hospital, Lahore, Pakistan
4 Dr. Amina Saeed Khan, Senior Registrar, Department of Neurology, Services Hospital, Lahore, Pakistan
Keywords:
NMDA encephalitis, Anti NMDA receptor
Full Text:
Introduction
Anti-N-methyl-d-aspartate (NMDA) receptor encephalitis is a rare autoimmune disorder caused by the formation of antibodies against the NMDA receptors in the brain [1]. A class of glutamate receptors called NMDA receptors is crucial for memory, learning, and brain development. These receptors, which may be found on the surface of neurons, allow specific substances, such as glutamate, to enter the cell. The development of antibodies against these receptors causes them to malfunction, which causes the encephalitis symptoms [2]. Although the precise cause for the development of these antibodies is unclear, it is considered to be connected to an underlying infection or tumor. Ovarian teratomas, which are benign tumors that can form in the ovaries, are sometimes linked to the condition [3]. Other times, no underlying reason can be identified.
The symptoms of anti-NMDA receptor encephalitis typically develop over a period of several weeks and can include confusion, hallucinations, seizures, memory loss, and difficulty speaking. Additionally, patients may develop autonomic dysfunction, such as changes in heart rate or blood pressure, as well as movement disorders, such as tremors or stiffness. Because the symptoms of the ailment frequently resemble those of a psychiatric problem, diagnosing the condition can be difficult. The diagnosis is typically made based on a combination of clinical findings, laboratory tests, and imaging studies.
Treatment of anti-NMDA receptor encephalitis typically involves administering immunotherapy, such as steroids or plasma exchange, to reduce inflammation and decrease the levels of antibodies [4]. In addition, any underlying infection or tumor must be treated. In some cases, a surgical procedure called a craniotomy may be required to remove a tumor that is believed to be causing the disorder [5]. Prognosis for patients varies depending on the severity of the disorder and the timing of treatment initiation [2,6]. Early diagnosis and treatment can lead to better outcomes, although long-term recovery may take months or years. The most reliable diagnostic method is detection of anti-NMDA receptor antibodies in cerebrospinal fluid (CSF) and serum using ELISA [7].
Case Presentation
An 18-year-old female patient presented to the Neuro OPD at Services Hospital Lahore, Pakistan with a week-long history of altered behavior, low grade fever, tonic posturing, and generalized rigidity. Altered behavior included visual hallucinations, aggression, irritation, disturbed sleep cycle, and crying spells. She also had difficulty recognizing family members and exhibited gestures as if catching objects in the air.
On examination, the patient's Glasgow Coma Scale (GCS) score was 12/15, with signs of meningeal irritation. Motor examination showed increased tone in all limbs and limb holding. Orofacial dyskinesia was noted. Other neurological and systemic findings were normal.
Laboratory and CSF analysis revealed elevated protein levels, lymphocytic pleocytosis, and normal glucose. MRI and EEG were initially unremarkable. Despite treatment with antivirals, antibiotics, steroids, and supportive therapy, the patient’s condition worsened, with increased seizure frequency and dysautonomia. Repeat MRI showed nonspecific white matter hyperintensities. Serum NMDA antibodies were strongly positive, confirming diagnosis.
The patient was treated with pulse therapy using injection solumedrol (1 g/day) for 5 days. Plasmapheresis was not feasible due to sepsis; therefore IVIG (0.4 g/kg/day for 5 days) was administered (Figure 1).
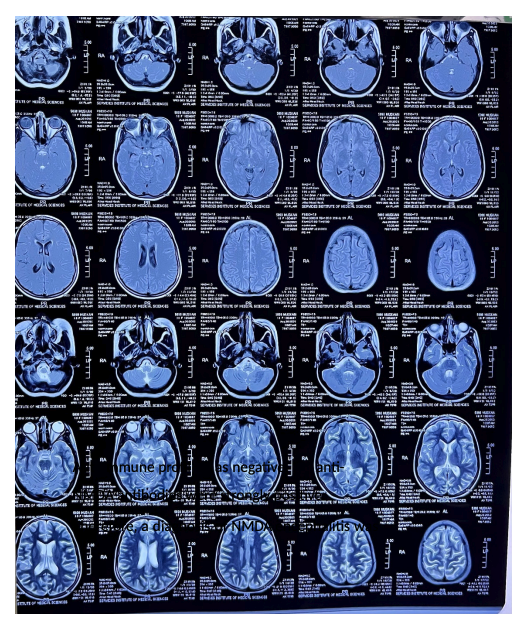
Figure 1. Aut mmune profil as negative, antiNMDA antibodies were strongly positive.
The patient showed significant improvement, achieving GCS 15/15 with reduced rigidity. She was discharged after one month on tapering steroids and azathioprine. Follow-up investigations showed no underlying etiology (Figure 2).
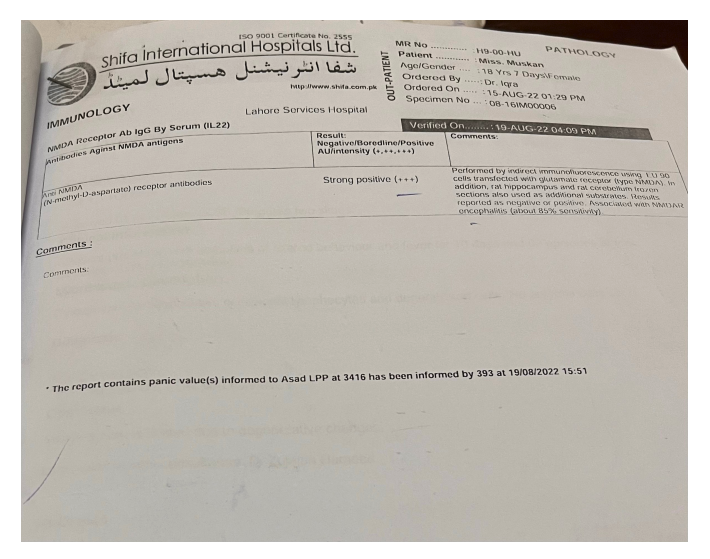
Figure 2. Serum immunology report showing strong positivity (+++) for anti-NMDA receptor antibodies.
Conclusions
Anti-NMDA receptor encephalitis is characterized by inflammation and antibodies against GluN1 subunits in CSF and serum [8]. It predominantly affects young individuals with a female predominance (1:4) [9]. The condition is often paraneoplastic [10], commonly associated with ovarian teratomas.
Diagnosis relies on antibody detection, CSF analysis, EEG, and MRI findings, although imaging may be normal in many cases [11]. Differential diagnoses include psychiatric disorders, infections, and drug-induced conditions. HSV infections may trigger anti-NMDA antibody production [12].
Treatment is individualized and includes immunotherapy and tumor removal when applicable. First-line therapies include corticosteroids, IVIG, or plasmapheresis [13] (Figure 3).
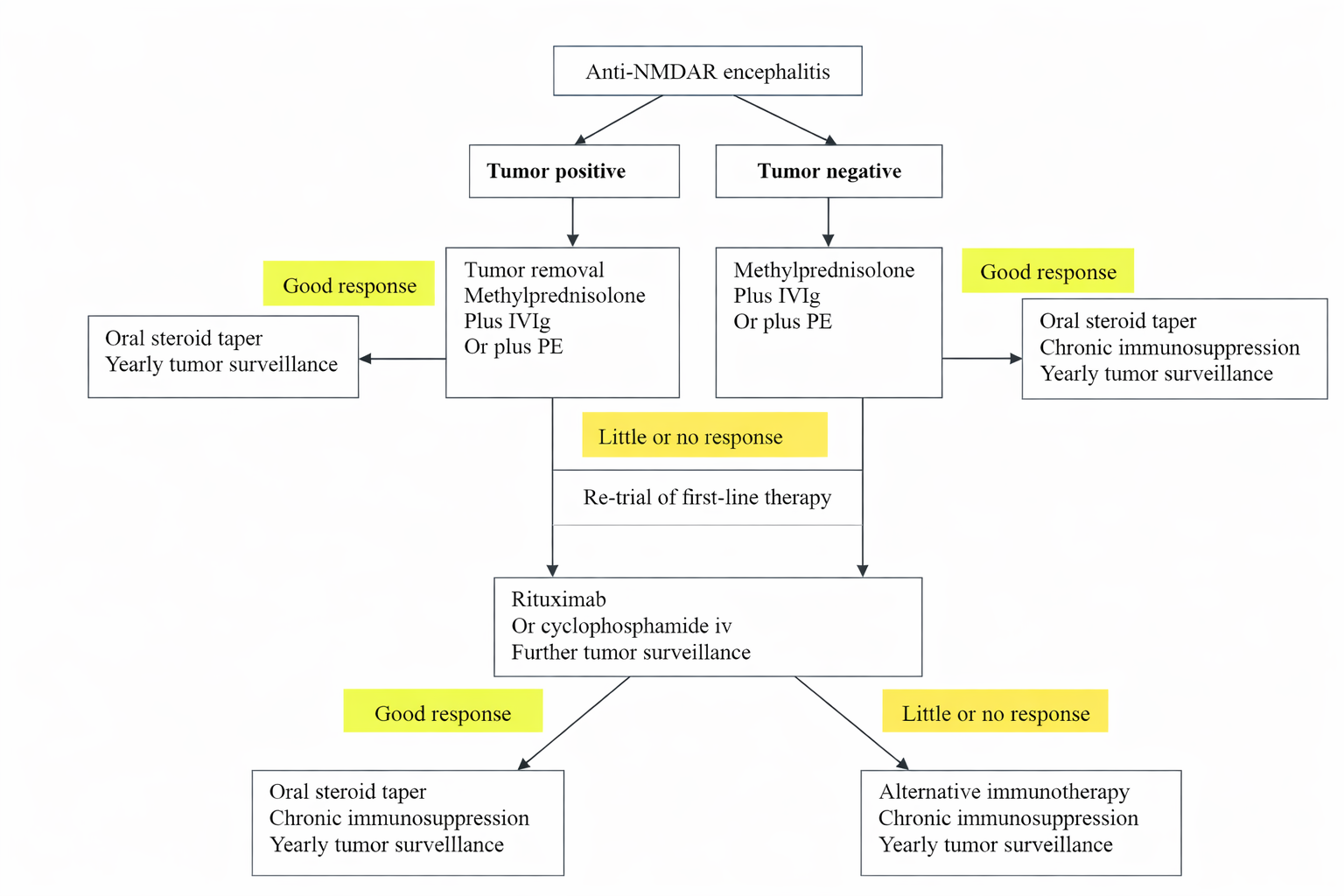
Second-line therapies include rituximab, cyclophosphamide, or mycophenolate mofetil, which has shown favorable efficacy and safety [14].
Disclosure
No conflicts of interest.
References:
References
Wang HY, Li T, Li XL, Zhang XX, Yan ZR, Xu Y. Anti-N-methyl-D-aspartate receptor encephalitis mimics neuroleptic malignant syndrome: case report and literature review. Neuropsychiatric Disease and Treatment. 2019;15(1):773-778.
Doi: https://doi.org/10.2147/NDT.S195967Huang Q, Xie Y, Hu Z, Tang X. Anti-N-methyl-D-aspartate receptor encephalitis: a review of pathogenic mechanisms, treatment, prognosis. Brain Research. 2020;1727(1):146549.
Doi: https://doi.org/10.1016/j.brainres.2019.146549Chiu HC, Su YC, Huang SC, Chiang HL, Huang PS. Anti-NMDAR encephalitis with ovarian teratomas: review of the literature and two case reports. Taiwanese Journal of Obstetrics and Gynecology. 2019;58(3):313-317.
Doi: https://doi.org/10.1016/j.tjog.2019.03.005Nan D, Zhang Y, Han J, Jin T. Clinical features and management of coexisting anti-N-methyl-D-aspartate receptor encephalitis and myelin oligodendrocyte glycoprotein antibody–associated encephalomyelitis: a case report and review of the literature. Neurological Sciences. 2021;42(3):847-855.
Doi: https://doi.org/10.1007/s10072-020-04979-2Forrester A, Latorre S, O'Dea PK, Robinson C, Goldwaser EL, Trenton A, Tobia A, Aziz R, Dhawan S, Brennan A, Kurukumbi M. Anti-NMDAR encephalitis: a multidisciplinary approach to identification of the disorder and management of psychiatric symptoms. Psychosomatics. 2020;61(5):456-466.
Doi: https://doi.org/10.1016/j.psym.2020.05.010Yang S, Yang L, Liao H, Chen M, Feng M, Liu S, Tan L. Clinical characteristics and prognostic factors of children with anti-N-methyl-D-aspartate receptor encephalitis. Frontiers in Pediatrics. 2021;9(1):605042.
Doi: https://doi.org/10.3389/fped.2021.605042Zhu J, Li Y, Zheng D, Wang Z, Pan S, Yin J, Wang H. Elevated serum and cerebrospinal fluid CD138 in patients with anti-N-methyl-d-aspartate receptor encephalitis. Frontiers in Molecular Neuroscience. 2019;12(1):116.
Doi: https://doi.org/10.3389/fnmol.2019.00116Barry H, Byrne S, Barrett E, Murphy KC, Cotter DR. Anti-N-methyl-d-aspartate receptor encephalitis: review of clinical presentation, diagnosis and treatment. BJPsych Bulletin. 2015;39(1):19-23.
Doi: https://doi.org/10.1192/pb.bp.113.045518Wilkinson-Smith A, Blackwell LS, Howarth RA. Neuropsychological outcomes in children and adolescents following anti-NMDA receptor encephalitis. Child Neuropsychology. 2022;28(2):212-223.
Doi: https://doi.org/10.1080/09297049.2021.1939197Rita CG, Nieto Gañan I, Jimenez Escrig A, Carrasco Sayalero Á. Anti-N-Methyl-D-Aspartate Encephalitis as paraneoplastic manifestation of germ-cell tumours: a case report and literature review. Case Reports in Immunology. 2019;2019(1):1-5.
Doi: https://doi.org/10.1155/2019/7014085Dalmau J, Lancaster E, Martinez-Hernandez E, Rosenfeld MR, Balice-Gordon R. Clinical experience and laboratory investigations in patients with anti-NMDAR encephalitis. Lancet Neurology. 2011;10(1):63-74.
Doi: https://doi.org/10.1016/S1474-4422(10)70253-2Lebon S, Mayor-Dubois C, Popea I, Poloni C, Selvadoray N, Gumy A, Roulet-Perez E. Anti-N-methyl-D-aspartate (NMDA) receptor encephalitis mimicking a primary psychiatric disorder in an adolescent. Journal of Child Neurology. 2012;27(12):1607-1610.
Doi: https://doi.org/10.1177/0883073812451325Nosadini M, Eyre M, Molteni E, Thomas T, Irani SR, Dalmau J, Dale RC, Lim M, Anlar B, Armangue T, Benseler S. Use and safety of immunotherapeutic management of N-methyl-D-aspartate receptor antibody encephalitis: a meta-analysis. JAMA Neurology. 2021;78(11):1333-1344.
Doi: https://doi.org/10.1001/jamaneurol.2021.3187Guan HZ, Ren HT, Cui LY. Autoimmune encephalitis: an expanding frontier of neuroimmunology. Chinese Medical Journal. 2016;129(9):1122-1127.
Doi: https://doi.org/10.4103/0366-6999.180518