The Journal of Neurology & Neuropsychiatry is a leading scientific publication dedicated to advancing the understanding and treatment of neurological and neuropsychiatric disorders. As a peer-reviewed journal, it serves as a platform for researchers, clinicians, and experts to share their latest findings, innovative methodologies, and clinical experiences in the field.
This journal encompasses a broad spectrum of topics, including but not limited to neurodegenerative diseases, movement disorders, epilepsy, neuropsychiatric conditions, and neuroimaging techniques. Its interdisciplinary approach fosters collaboration between neurologists, psychiatrists, neuroscientists, and other healthcare professionals, contributing to a holistic understanding of the complexities of the brain and mind.
The Journal of Neurology & Neuropsychiatry prioritizes high-quality research that enhances diagnostic accuracy, treatment efficacy, and patient outcomes. Through the publication of original research articles, review papers, and case studies, the journal provides a comprehensive overview of the latest developments in neurology and neuropsychiatry.
Researchers and practitioners alike rely on the journal to stay informed about emerging trends, novel therapeutic interventions, and breakthroughs in neuroscientific research. The Journal of Neurology and Neuropsychiatry plays a crucial role in advancing the field, shaping clinical practices, and ultimately improving the lives of individuals affected by neurological and neuropsychiatric conditions.
| Field | Details |
|---|---|
| Title | Journal of Neurology & Neuropsychiatry |
| ISSN | Applied |
| Established (ESTD) | 2024 |
| Subject Category | Neurology, Neuropsychiatry, Brain Disorders |
| Issue Frequency | Quarterly |
| Publication Format | Fully Open Access |
| Language | English |
| Publisher Details | CLS Event & Publication |
Giuseppe Bonavina1*, Monika Zackova1, Erik Del Mestro2, Alice R. Portillo3

Juliana Bezerra Lima-Verde1, Annamaria Gomes Pereira1 and Jair Soares dos Santos1*

Levin Ace Danganan1*, Elizer Montemayor1, Renato Dejan Jr.1
Ulziizaya Sodov1*, Tovuudorj Avirmed1, Khishigsuren Zuunnast1
Valentina Colombo1*, Pamela Salucci1, Francesca Cesira Cava1, Giuseppe Bonavina1, Alice Rita Portillo1, Elisa Maietti2, Roberto Piperno3

Safaa K. H. Khalil1, W. El hotaby1, Gehan. A-R Ahmed1*, Gihan Kamel2,3 , Hadeer H.A. Sherif1, Lamyaa Abbas1
Sabina Nayab1*, Qasim Bashir2, Adnan Aslam3, Amina Saeed khan4
Paula Abola 1,*, Benjamin Wolden 1 and Mitchell Wolden1
Journal of Neurology & Neuropsychiatry, an open-access, peer-reviewed publication, welcomes submissions covering the entire spectrum of neurological disorder prevention, diagnosis, and treatment. Additionally, it explores topics related to molecular genetics, pathophysiology, and epidemiology in this field.
The preoperative evaluation of the function of vital organs including heart, lungs, liver and kidney is established practice across all surgical specialities. Effective perioperative evaluation and optimization has been shown to reduce postoperative medical complications, but nowadays there is a gap in the perioperative evaluation of neurological status [1]. Brain health is largerly overlooked by current modalities of perioperative assessment. On the other hand, existing protocols and guidelines focusing on modifiable risk factors for cardiac, pulmonary, renal, and metabolic-related complications have clearly demonstrated that prehabilitation strategies can decrease not only complication rates, but also 30-day mortality and length of hospital stay [2]. Frailty in the elderly population is strongly associated with the risk of postoperative complications, delirium, institutionalization, and mortality. Delirium remains the most common postoperative adverse event, with a pooled risk ratio of 2.13 (95% CI 1.23-3.67), but it can also be a marker of preclinical dementia and may contribute to delayed neurocognitive recovery [3]. It is indeed time to appreciate that surgical stress and systemic inflammation may lead to neuroinflammation, worsen preoperative neurologic status, and increase neurological complication rates in vulnerable individuals who lack physiological reserve and present with multisystemic functional deterioration. Use of Electroencephalography (EEG) monitoring as a guide to anesthetic titration to reduce the rate of perioperative cognitive disorders may prove a useful adjunct in this category of patients, but it is currently under investigation [4]. EEG is essential for differentiating delirium (a state of usually reversible global brain disfunction) and seizure disorders (a condition of spontaneous, recurrent paroxysmal electrical dysfunction), enabling the distinctly different treatment: Antiepileptic Drugs (AEDs) are a class of medications that have indeed received considerable attention as possible treatments for agitation and aggression, despite a lack of high-quality data and despite neurologist and psychiatrist often disagree on terminology.We believe that preoperative assessment of elderly and frail patients is often neglected in everyday practice but remains the foundation for a safe surgical practice. In United Kingdom, the proactive care of older patients undergoing surgery (POPS) model has integrated the Comprehensive Geriatric Assessment (CGA) in the elective and emergency surgical setting, and has provided a robust evidence based methodology to identify the elderly population at risk and to optimize the surgical pathway and the follow-up after hospital discharge [5]. A randomized clinical trial showed that preoperative CGA and optimization according to the POPS model result in fewer non-surgical complications and reduce the length of hospital stay by 40% compared to standard care [6].Normal Pressure Hydrocephalus (NPH), a condition most commonly seen in older adults is often misdiagnosed (less than 20% of patients in a Neurological unit receive an appropriate diagnosis) but has emerged as a “treatable movement disorder”, and represents a cause of delirium or cognitive decline in elderly adults who undergo cardiac surgery [7].An important aspect of perioperative care is that several drugs may have a significant impact on neurological perioperative outcomes, especially in elderly patients in whom polypharmacy is common practice. Multiple prescriptions and non-prescription medications have the potential for drug-to-drug interaction and perioperative adverse events. Although electronic health records have the potential to detect errors and interactions, having the patient bringing in all medications they use at home is a critical step at the time of office visit to prevent adverse outcomes due to drug abuse, withdrawal or interactions. Many group of drugs can cause delirium and this includes many prescriptions over the counter, complementary (“natural”) and alternative products (some examples of herbal products that have cholinergic effects are henbane, jimson weed and mandrake and some teas). The mechanism of drug induced delirium are not well defined, but evidence support a major role for cholinergic failure. Anticholinergic intoxication causes a classical delirium syndrome that may be reversible with cholinesterase inhibitors; drugs which can cause a muscarinic blockade can leads to delirium and drugs such as digoxine, lithium and histamine (H2) antagonists shoes measurable cholinergic receptor binding. The most common drugs associated with delirium are sedative hypnotics (benzodiazepines), analgesic, and medications with an anticholinergic effect. Serotoninergic drugs may also indirectly contribute to delirium by causing serotonin syndrome (in particular paroxetine due to greatest affinity for muscarinic receptors), and neuroleptic malignant syndrome [8]. This reciprocal relationship between cholinergic and dopaminergic brain effects indicate a role for dopaminergic excess in delirium and explain why dopaminergic medications such as levodopa or dopamine agonist can contribute to delirium in a dose related manner. Dopamine dysregulation syndrome and punding are encountered with levodopa therapy particularly if delivered in an intermittent fashion, with slow-release formulations and it it’s crush a slow release formulation in a nasogastric tube, as levodopa competes with amino acids for uptake in proximal small intestine. Even gastric emptying can result in erratic absorption and bioavailability. For these necessary medications, a dosage reduction or adjusting the dosage schedule may be helpful; for example, if antiparkinsonism medications are suspected of causing confusion, anticholinergic medications should be the first to be discontinued, followed by selegiline, dopamine agonist and finally and most important, by tapering levodopa, as many patients can develop an acute “akinetic attack” with hyperpyrexia and diaphoresis resembling the clinical picture of neuroleptic malignant syndrome that it may follow an abrupt change in dopaminergic medication [9-13]. Also, use of herb medications should be carefully reviewed. Patients should be counselled and monitored regarding pharmacological therapy in preparation for the surgical procedure. Deprescribing may be necessary, and alternative routes for neurotropic drug administration should be considered in the immediate postoperative period, especially after foregut procedures that may transiently impair the ability to swallow or bowel absorption.Concurrent medical problems may also contribute to “drug induced delirium”, for example in heart failure, hepatic insufficiency and renal failure; antibiotics mainly cephalosporins and macrolids may induced delirium; the mechanism behind this phenomenon is still not fully understood but has been hypothesized that may lower the seizure threshold by binding competitively to the GABA-A receptor inducing a Non-Convulsive Status Epilepticus (NCSE) manifested by an altered mental state. Frailty, rather than chronological age, is increasingly recognized as a predictor of adverse postoperative events. Interestingly, a large cohort study conducted across 9 noncardiac specialties showed that there was a greater than 10% 180-day mortality for frail patients following even low- stress procedures in low-intensity specialties [6]. This confirms that triage and optimization of preoperative assessment should be mandatory for all surgical specialties regardless of the planned procedure. Furthermore, it is time to expand the concept of pre-habilitation to include optimization of neurological functional status among the therapeutic targets. It is possible that screening for depression, anxiety, movement disorders and stroke, and a period of structured cognitive exercise along with pharmacological modulation, if necessary, can help to identify reversible deficits and strengthen the capacity of the patient to withstand surgical stress. In stroke and many neurological disorders there is impaired integrity of blood-brain barrier function, which allows more of a potentially toxic drug to reach the brain and reduced integrity of blood-brain barrier function is strongly associated with susceptibility to delirium. A comprehensive evaluation of the neurological status in elderly patients who are surgical candidates and the adoption of a collaborative neuro- geriatric perioperative care pathway could fill an existing gap, and successful treatment of delirium depend on identifying the reversible contributing factors, as drugs are the most common reversible cause of delirium. Some recent studies suggest that dexmedetomidine , a sympatholytic drug that acts as agonist to alpha-2-receptor, use for sedation in mechanically ventilated adults may reduce time to extubation in neurological disorders, may be associated with less delirium and appears to be associated with less neurocognitive dysfunction compared to other sedatives, but these findings were inconclusive because of publication bias, heterogeneity and limited sample size. These factors can improve current modalities of anesthesiological and surgical risk stratification, and reduce the risk of postoperative cognitive disorders and functional decline [11]. Finally, discharged patients form intensive care to general ward have a better neurological outcome and less subclinical delirium using the “ABCDE bundle” (Awakening and breathing coordination, delirium monitoring and exercise/early mobility”): we should investigate better if ward-transfers, arriving in the Emergency Department (ED) at nighttime, time spent in ED and visits from other specialists at nighttime could be possibly associated with development of “incident delirium” and delirium motor subtypes; the transfer of patients from the Intensive Care Unit (ICU) to a general ward can present several challenges, ensuring optimal care and reducing delirium; let us change our attitude as neurologists and clinicians, “from bed to wheelchair” [12].
This is a letter to the editor of the journal aimed at highlighting the importance that Generative Reprocessing Therapy (TRG) has gained in the last two years through the resolution of clinical cases of individuals with depression, anxiety, suicidal ideation, or fibromyalgia that have been published and report situations resolved by TRG. The reports demonstrate the effectiveness that TRG has had in improving the quality of life of these patients, where many have undergone medication tapering for these purposes. TRG has been shown to be an alternative for those cases of individuals with depression, anxiety, suicidal ideation, or fibromyalgia that cannot be resolved through conventional therapies. Further research is being conducted to better understand how this therapy works in restoring mental health.
Background: Guillain-Barre Syndrome is a debilitating neurological disease with an incidence of 1.1 - 1.8 per 100,000. Autoantibodies affecting peripheral nerve membranes play an important role in understanding the pathophysiology and treatment of it. Treatment options for its cure continue to unfold and evolve. Different clinical trials resulted in increased interest in therapeutic apheresis for treatment of severe and refractory disease.Objectives: Conflicting results of immunoadsorption compared to plasma exchange in the management of Guillain-Barre Syndrome led us to synthesize available evidence from published studies. METHODS: Review Manager software was used for this review and classified the outcomes into primary (curative effect) and secondary (safety profile and relapse rate). Quality assessment and statistical data analysis were conducted using the said software.Result: The odds of achieving at least one grade disability and functional improvement was similar for patients treated with immunoadsorption and plasma exchange (OR: 0.77; 95% CI: 0.34 - 1.74; p = 0.53). Reduced risk of complications for patients treated with immunoadsorption group as compared to plasma exchange group (RR: 0.69; 95% CI: 0.43 - 1.11; p = 0.13) was noted. Increased risk of relapse for patients who underwent immunoadsorption (RR: 1.70; 95% CI: 0.96 - 3.00; p = 0.07).Conclusion: Immunoadsorption is at least as effective as plasma exchange in the treatment of Guillain-Barre Syndrome based on its curative effect by lowering its disability and improving functional score. Immunoadsorption showed reduced complications but relapse rates were higher compared to plasma exchange.
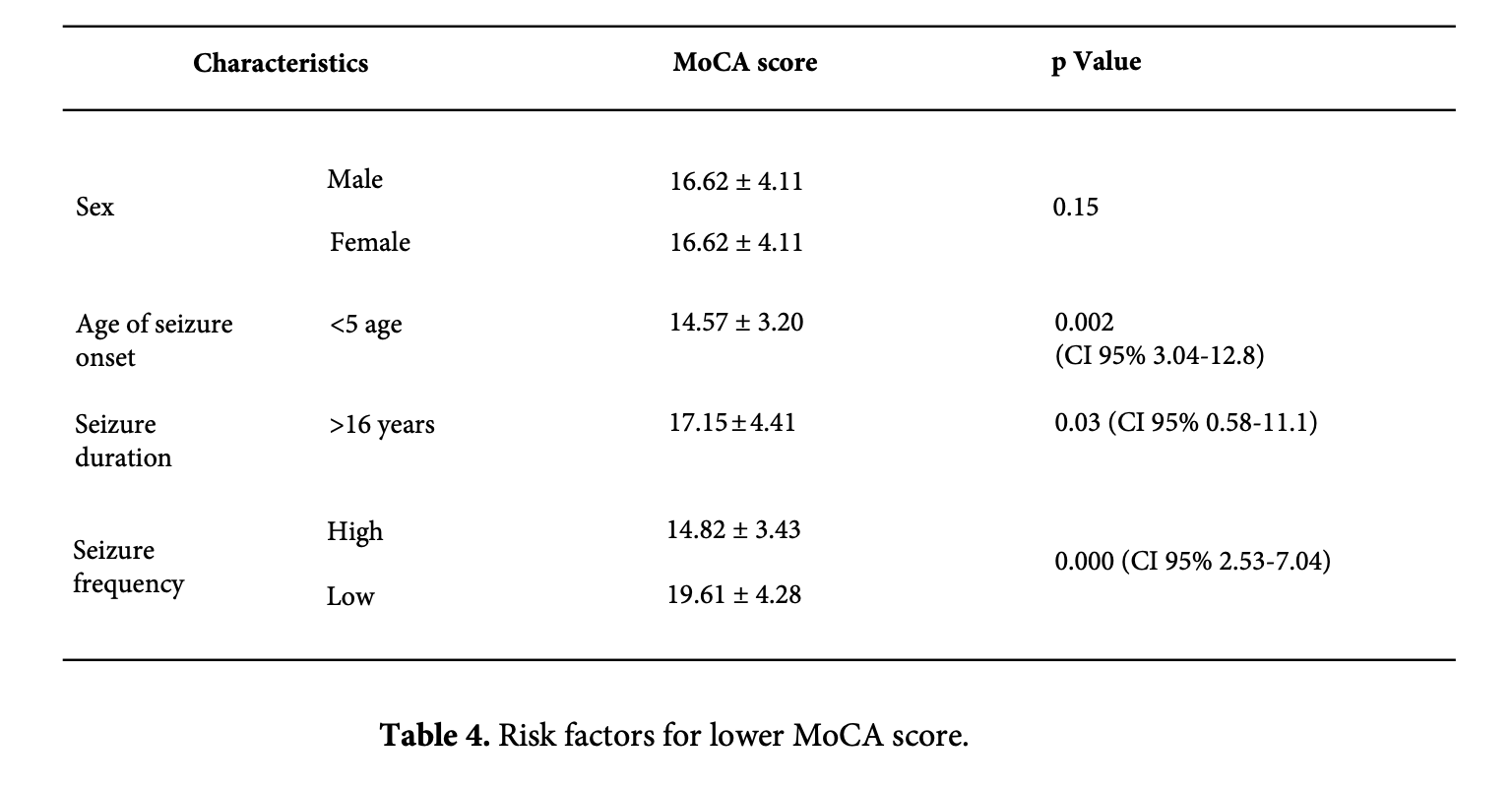
Introduction: Focal epilepsy accounts for 60% of all clinical epilepsy cases, while temporal lobe epilepsy (TLE) accounts for 40%. Cognitive impairment such as language, attention, executive function, and memory impairment are common in temporal lobe epilepsy, and researchers believe that seizure frequency and duration can cause severe hippocampal sclerosis, as well as a secondary impact on neuronal metabolism and structure, which leads to cognitive impairment. Aim: The goal is to determine the cognitive impairment of temporal lobe epilepsy, the clinical characteristics and risk factors. Materials and Methods: A cross-sectional study of 50 adults with temporal lobe epilepsy from the National Center for Mental Health used a questionnaire and Montreal Cognitive Assessment (MoCA). Results: We included 50 adults aged 26 to 61 with temporal lobe epilepsy, 52% of respondents were male, 48% were female, with an average age of 43.78±8.20 years. The study found that 92% of individuals showed cognitive impairment, with mean MoCA scores of 17.50±4.57. Long lasting seizure is a high-risk factor for cognitive function, with statistical significance (p=0.03). Seizure onset age was linked with increased attention impairments and poor visuospatial function (p=0.005), while higher seizure frequency was associated with decreased calculation (p=0.04), language (p=0.009), and drawing skills (p=0.013). Conclusion: Our study found that 58% of respondents showed moderate cognitive impairment. Low education level, earlier age of seizure onset, high seizure frequency, extended seizure duration, presence of aura, and refractory temporal lobe epilepsy all have a statistically significant effect on cognitive impairment.

AimOur study investigates the link between neuroinflammation in the olfactory bulb (OB) and Parkinson’s Disease (PD). We aim to understand how environmental factors, such as viruses and particles, trigger a cascade of events leading to ?-synuclein aggregation and the development of PD.MethodsWe conducted histological studies of PD brains, pinpointing ?-synuclein abnormalities in the anterior olfactory structures at Braak's stage 1. Our study expanded post-mortem examinations to include the OB. We assessed:The vulnerability of the olfactory epithelium and OB to inflammation, considering age-related epithelial changes.The role of microglia in the OB and their potential as a barrier against exogenous pathogens.The entry of toxins, viruses, and nanoparticles into the OB, using animal models.ResultsOur research highlights the association between viral infections and PD, including the 1918 influenza pandemic and childhood infections. Chronic rhinitis and the presence of influenza A virus in PD brains further support this link.Animal studies reveal the impact of neurotropic viruses entering via the olfactory route, leading to ?-synuclein aggregation and widespread inflammation.Activated microglia play a pivotal role in pathogen clearance but also disrupt the blood-brain barrier (BBB), particularly in the OB.Metal particles such as aluminum and iron were identified as potential contributors to PD through chronic inflammation.ConclusionThis study unveils the critical role of OB neuroinflammation as a trigger for PD. Environmental factors significantly influence PD pathogenesis, offering potential avenues for intervention and prevention. Our findings enhance the understanding of this neurodegenerative disease and open new prospects for future PD research and treatments.

SMART-ID is a widely used digital authentication application in Latvia, enabling secure access to online banking, government portals, and healthcare services [1]. While its speed and convenience have benefited the general population, its current design may unintentionally exclude a vulnerable user group: individuals living with Parkinson’s Disease (PD).In informal discussions with several people diagnosed with PD, a recurring issue was raised concerning the difficulty of entering the required PIN code in the SMART-ID app. Parkinson’s-related hand tremors, a common motor symptom, often lead to accidental mistypes during PIN entry [2]. Since the app automatically processes the code as soon as it is entered, users are not given the opportunity to review or confirm the code before it is validated. After a few incorrect attempts, the app is locked, resulting in loss of access and the need for time-consuming reactivation steps, often with assistance from others.Although the SMART-ID app complies with high security standards, current accessibility practices suggest that authentication systems should offer alternative input options or confirmatory steps to accommodate users with motor impairments [3,4]. I have contacted the SMART-ID development team and suggested a small but potentially impactful modification: introducing a manual confirmation step (e.g., an “OK” button) after PIN entry. This would allow users with motor difficulties to verify or correct their input before the system registers a failed attempt. For individuals with PD, such a design improvement could significantly reduce frustration, prevent lockouts, and promote digital independence. As healthcare systems become increasingly digitized, we must ensure that authentication tools are inclusive of those with physical or neurological disabilities [5]. While this issue may seem minor from a system perspective, it has meaningful implications for quality of life, autonomy, and equitable access to essential services.I hope this suggestion will encourage developers and digital health policymakers to consider accessibility-enhancing features in authentication apps, not only in Latvia but globally.
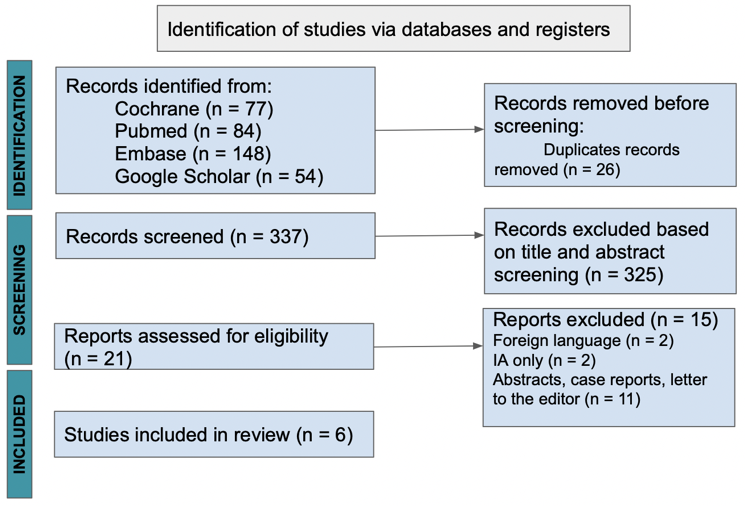
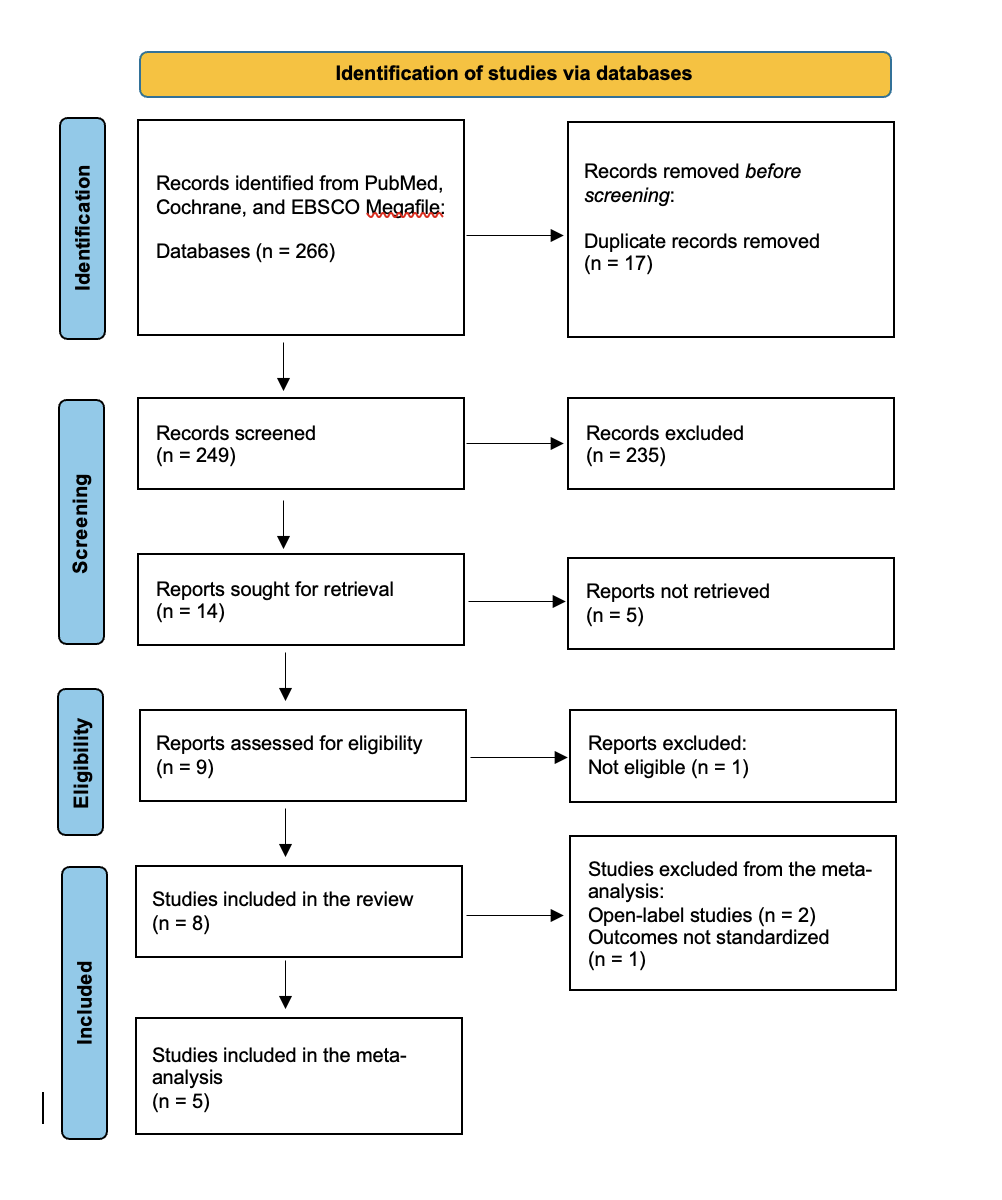
Background: Parkinson’s Disease (PD) is a progressive neurodegenerative disorder characterized by motor fluctuations and dyskinesias that become increasingly challenging to manage in advanced stages. Continuous subcutaneous Apomorphine infusion offers a less invasive alternative to device-aided therapies such as deep brain stimulation and Levodopa-Carbidopa intestinal gel. This systematic review and meta-analysis aimed to evaluate the efficacy of Apomorphine infusion in reducing OFF time and motor symptom severity, focusing on Unified Parkinson’s Disease Rating Scale (UPDRS) Part III scores in individuals with advanced PD. Objectives: A systematic search of PubMed, Cochrane, and EBSCO Megafile databases was conducted through April 16, 2025, according to PRISMA guidelines. Randomized controlled trials (RCTs) evaluating Apomorphine infusion and reporting outcomes on OFF time and UPDRS Part III were included. Risk of bias was assessed using the Cochrane RoB 2 tool, and certainty of evidence was evaluated with GRADE. Meta-analyses were performed using a random effects model. Result: Eight studies (n = 458) met the inclusion criteria, of which five were eligible for meta-analysis. Apomorphine infusion significantly reduced OFF time compared to placebo (MD = -1.93 hours; 95\% CI: -2.91 to -0.95; low-certainty evidence), with minimal heterogeneity (I² = 0\%). A significant reduction was also observed in UPDRS Part III scores (MD = -19.11; 95\% CI: -25.54 to -12.68; very low-certainty evidence), although substantial heterogeneity was present (I² = 67.93\%). Conclusion: This systematic review supports the efficacy of Apomorphine infusion in reducing OFF time and improving motor symptoms in individuals with advanced PD. Apomorphine infusion represents a treatment option, particularly for patient’s ineligible for surgical interventions. However, the overall certainty of evidence is limited by methodological heterogeneity and a small number of high-quality trials. Future studies should aim for standardized outcome measures, long-term comparisons with other device-aided therapies, and exploration